The US Political System Is to Blame for This Pandemic
Donald Trump richly deserves to be condemned for his response to COVID-19. But the catastrophic failures of public policy didn’t start with Trump: this bipartisan disaster has been decades in the making.
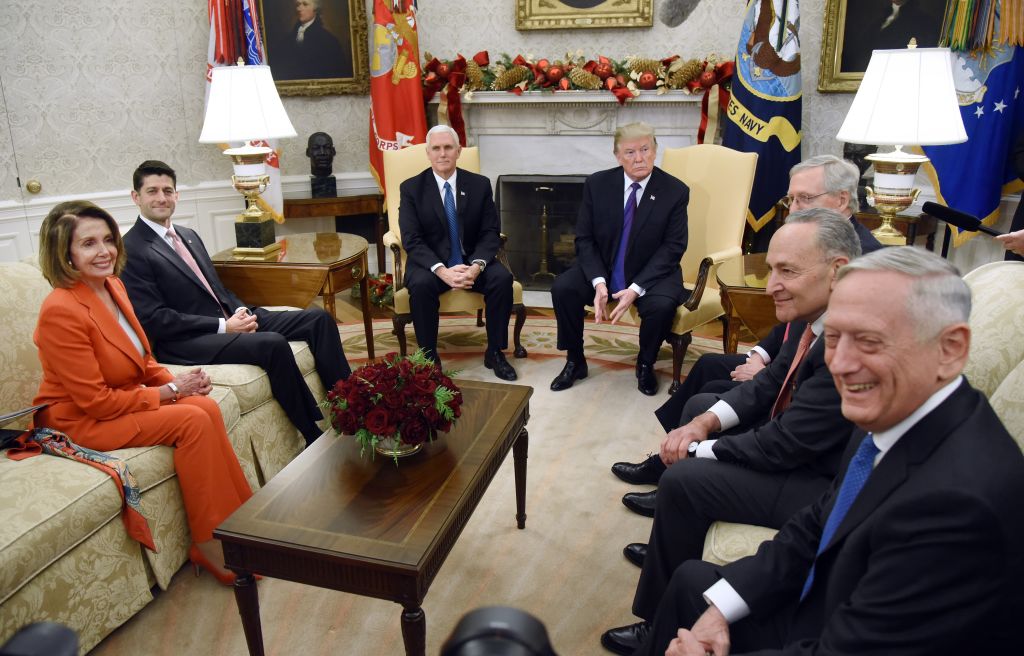
President Donald Trump and Vice President Mike Pence meet with Congressional leadership including Nancy Pelosi and Mitch McConnell in the Oval Office of the White House on December 7, 2017 in Washington, DC. (Olivier Douliery / Getty Images)
When historians ask why the United States became the world’s epicenter for the coronavirus, the temptation will be to blame it all on Donald Trump. After all, why wouldn’t they?
Trump disbanded the National Security Council’s pandemic response team in 2018. He scrapped an early warning program for pandemics just three months before the current outbreak. Most of his appointees who had been briefed on possible scenarios by outgoing Obama officials fell victim to his administration’s record-breaking turnover rate. And despite having been repeatedly warned about the virus, not least in his January intelligence briefings, Trump played down its severity for months, fatally misinforming his supporters, and even held rallies.
Since Trump finally decided to take the pandemic seriously, his response has been halting, chaotic, and even vindictive, seemingly withholding aid to Democratic state governments, while stepping it up for Republican ones. When the history of the pandemic is written, Trump will justifiably get the lion’s share of blame for possibly hundreds of thousands of deaths that the United States is predicted to see.