Coal Miners’ Struggle Against Black Lung Is a Climate Justice Issue
Climate activists often argue that carbon-intensive energy like coal is mortgaging our future. It’s true — but coal workers themselves have already been paying the costs for a long time, measured in hundreds of thousands of shortened lives ravaged by diseases like black lung in the US alone.
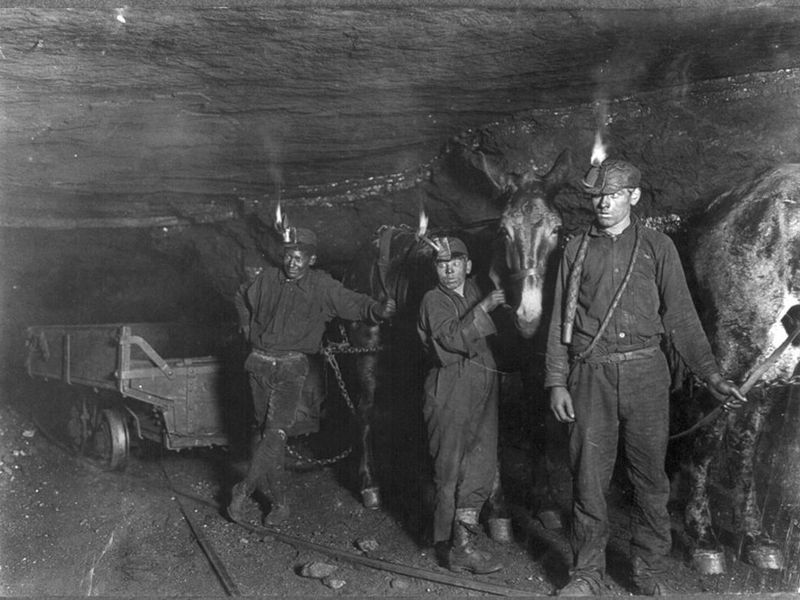
Coal miners with mules in Gary, West Virginia in 1908. (Library of Congress)
Carl Michelbacher had been disabled for years with black lung, a fatal respiratory disease caused by inhaling coal dust, when he appeared before the Senate Subcommittee on Labor in the winter of 1969. He was only fifty-nine, and he and his wife had five children under the age of eighteen. Unable to work and struggling to draw breath, he had struggled to piece together a patchwork of support: $337 each month from Social Security, a monthly union pension of $115, and biweekly payments of $95 under Pennsylvania’s workers’ compensation system, at the time one of the few state systems which recognized black lung. But when Senator Harrison Williams (D-NJ) asked him to provide his personal observations to the committee, Michelbacher replied, “I am just one of the lucky ones.”
Williams was stunned and asked Michelbacher to repeat himself. How could a middle-aged man, totally disabled with a preventable occupational disease that would eventually kill him, consider himself lucky?
When pressed to elaborate, Michelbacher pointed to his relative financial stability compared to other miners dying from the disease. He fell into a narrow window of black lung claimants at the time who were able to collect both workers’ compensation and Social Security. Qualifying for both was nearly impossible, and more recent claimants who managed to qualify had their workers’ compensation deducted from their Social Security.